


01
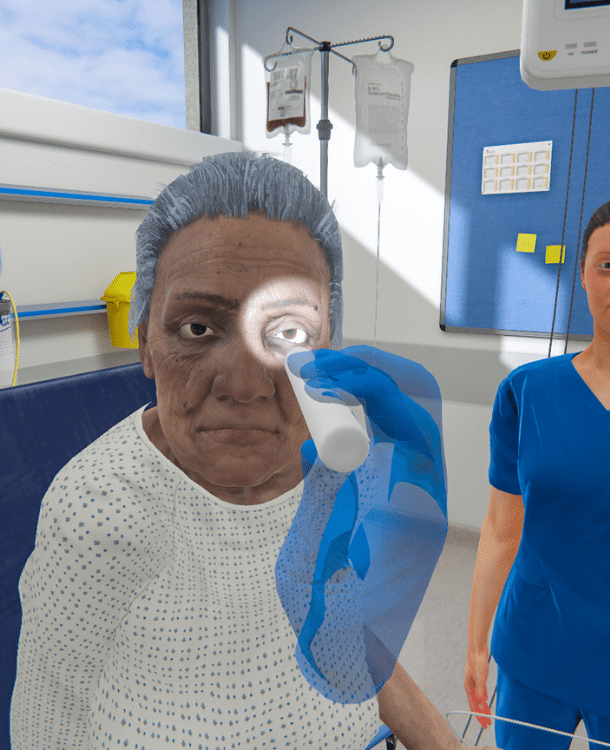
Depth and breadth
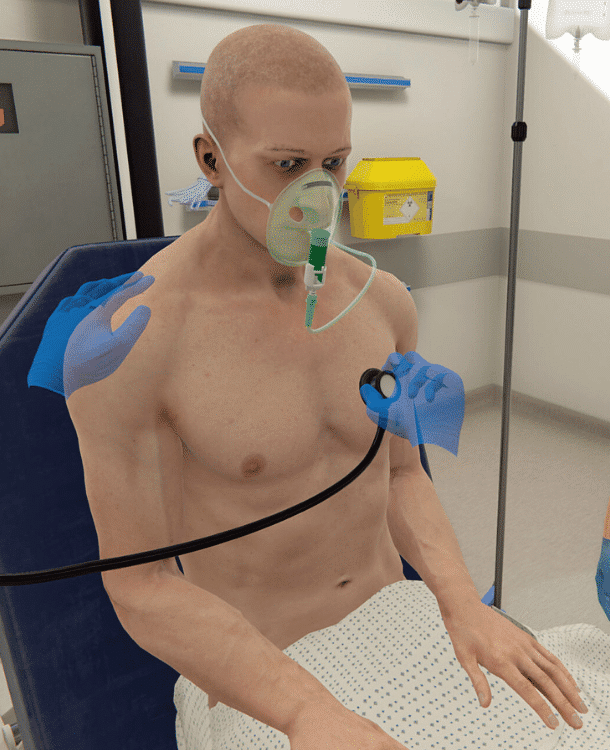
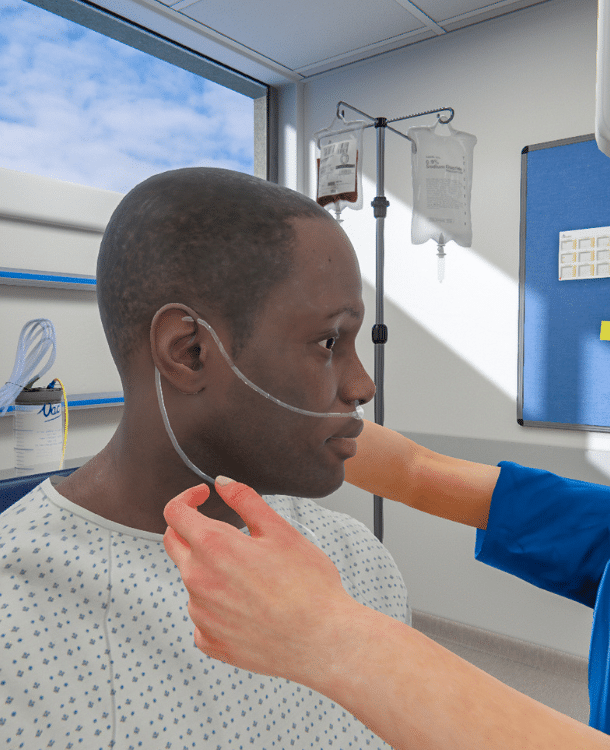
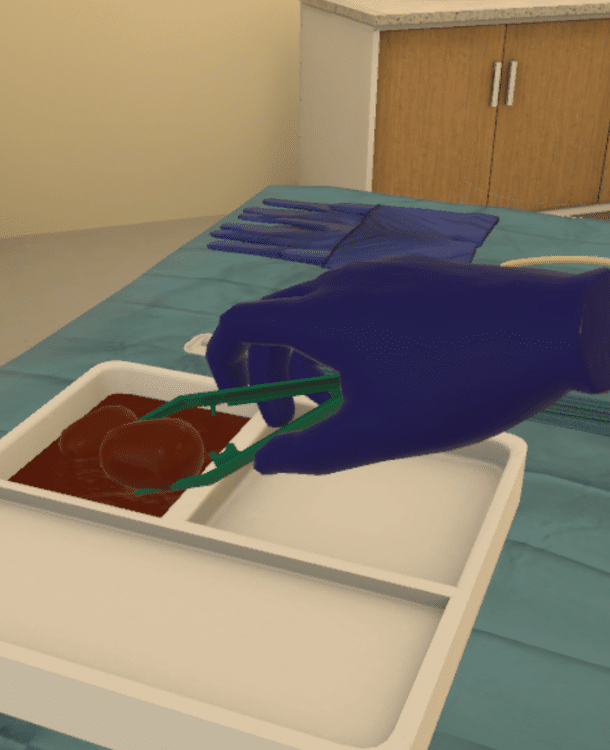
240+ scenarios across nursing, medicine, and allied health from fundamentals to ACLS
02
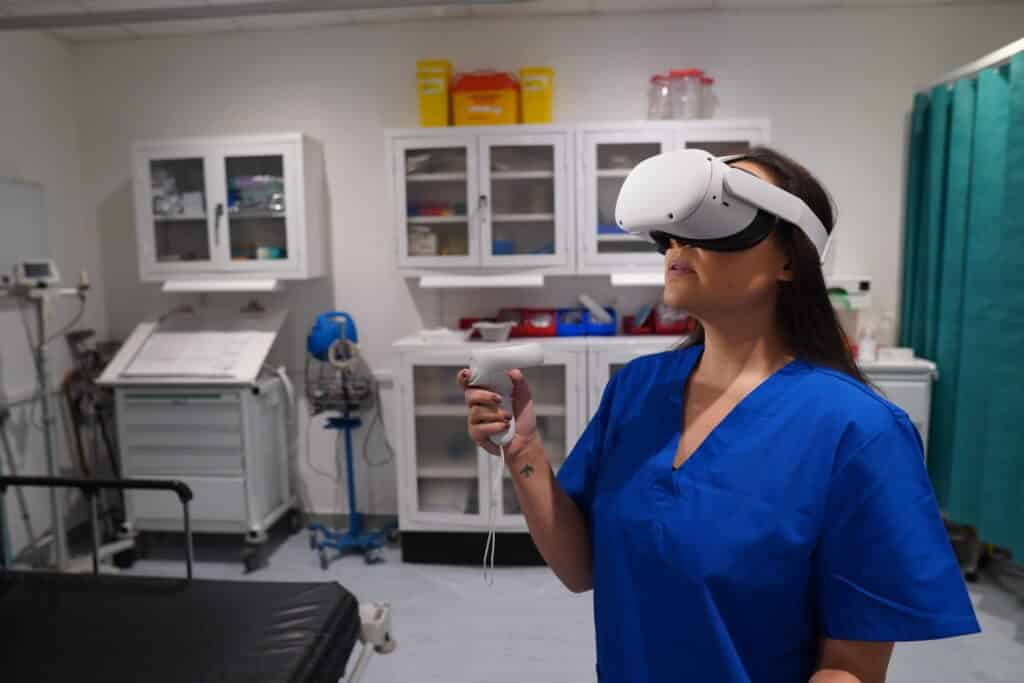
Instant scalability
Automated scenarios in VR and on screen offer simulation at scale and standardize clinical experiences
03
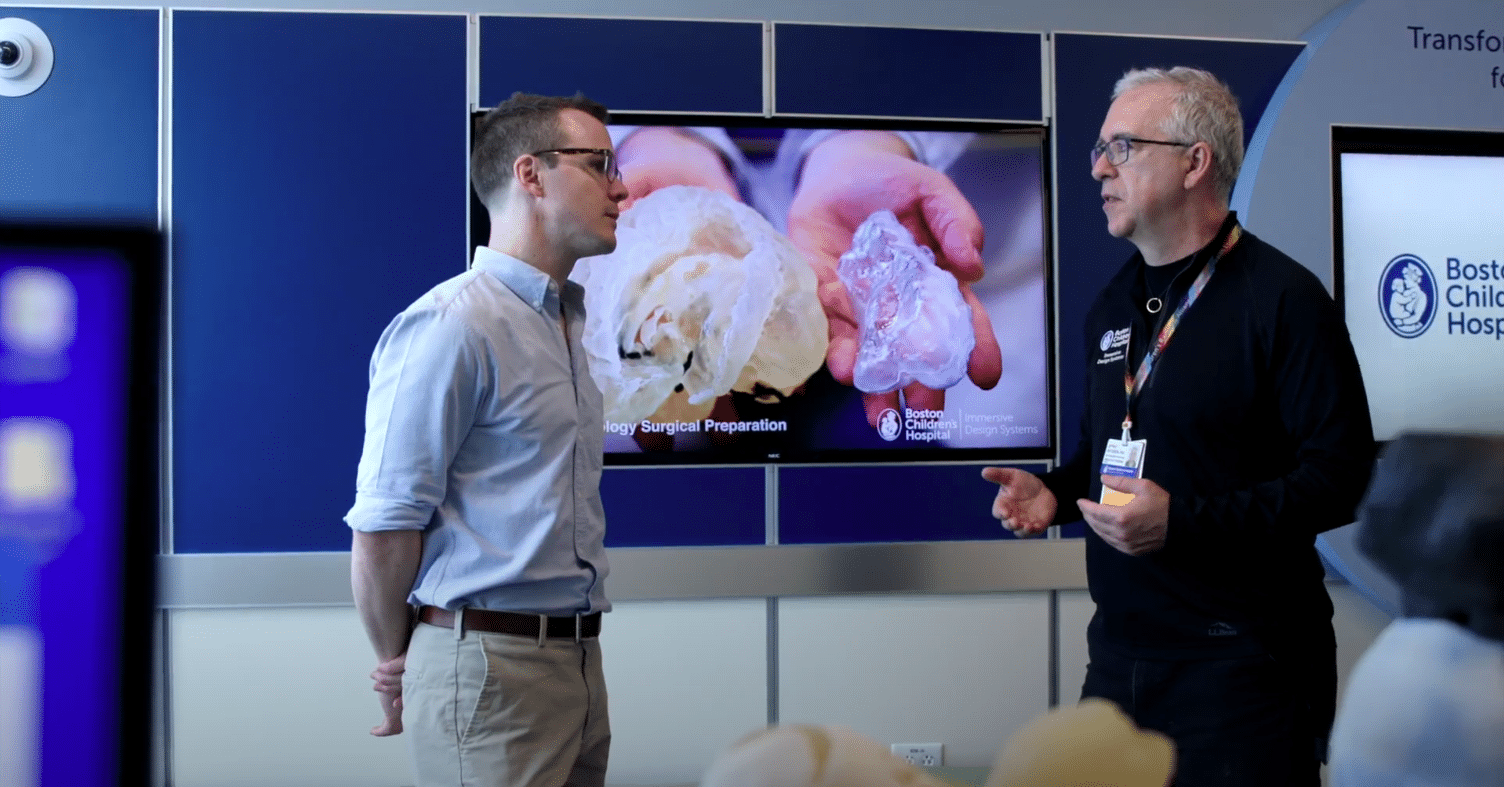
Customize as needed
No-code authoring platform allows you to adapt scenarios to meet your unique needs
04
Expert feedback
Immediate, evidence-based performance feedback written by clinicians, for clinicians
05
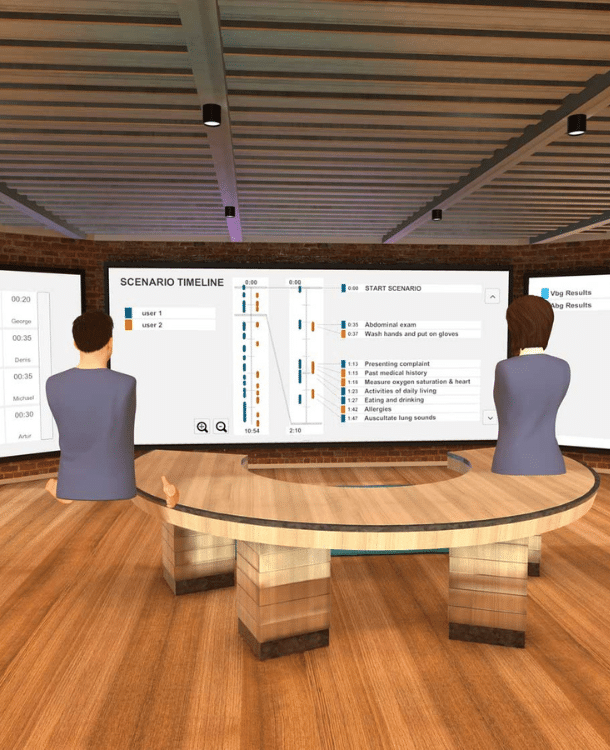
Precision analytics
Track progress, identify trends, and remediate issues with objective performance data
06
We're with you
Dedicated onboarding and success team with you every step of the way
07
Meet any need
Individual, multiplayer, hand interaction, voice control, and multi-patient scenarios