Virtual Reality Medical Training
-
-
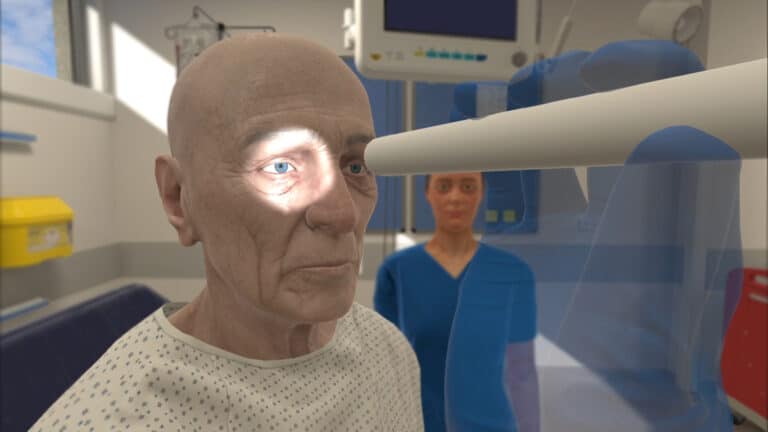
Using Your Voice: Communicating with AI-Driven Virtual Patients
What does it truly mean for a learner to be ready – and are we doing enough to get them there?
-
Virtual Reality: A New Wave for Simulation-Based Education
Whether in the classroom or the clinical setting, opportunities for learners to practice skills freely and in a safe environment are limited. However, replicating real-world clinical scenarios is crucial in preparing students for practice and reinforcing knowledge and skills for clinicians. This recreation of specific clinical situations is often referred to as ‘simulation-based education’, and…
-
Leveraging Virtual Reality to Improve Maternal Care
Preparing for the arrival of a new baby is often a time filled with joy, love, and anticipation as soon-to-be parents get ready both physically and mentally for a new chapter of life. While pregnancy should be a time devoted solely to the excitement of bringing in new life, it sadly continues to be a…
-
The True Cost of Nursing Turnover: Why Nurses are Resigning and What It Means for the Healthcare Industry
Nursing has seen a shift in recent years that has caused alarm – higher turnover rates, staff shortages, and an increased demand for healthcare professionals have impacted the remaining staff and patients. It’s significantly financially costly for hospitals to replace lost staff, not to mention the time and resources cost of finding a suitable replacement….
-
Oxford Medical Simulation Raises $12.6 Million in Series A Funding to Address Critical Healthcare Training Gap with Virtual Reality
Talking with a patient is one of the best ways for healthcare professionals to hone their communication skills – gathering history, explaining rationale, building rapport, or even having difficult conversations.
-
Healthcare Simulation | Interprofessional VR Simulation | Uncategorized | Virtual Reality Medical Training
OMS for Interprofessional Team Building
Building a safe space for a working environment is imperative to interdisciplinary team success in healthcare settings. VR can be used as a way to connect the interprofessional team from any space, providing similar benefits to that of in-person team building simulations.
-
Oxford University Partners with Oxford Medical Simulation
Oxford University has partnered with Oxford Medical Simulation to train medical students using virtual reality.






End of content
End of content
