EKG (ECG) Interpretation
Maria, Sinus tachycardia with peaked T waves [SIE002US]
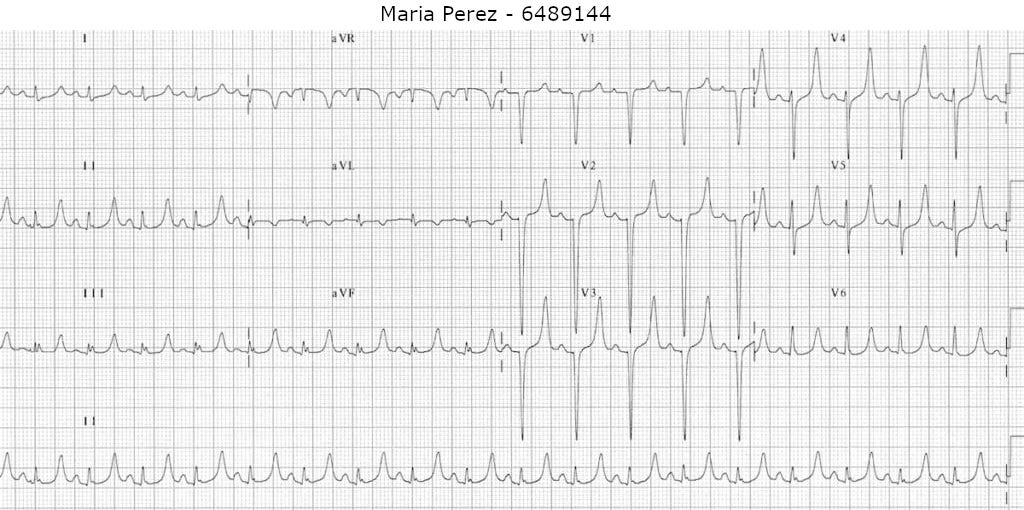
This is the EKG (ECG) for Maria Perez from scenario SIE002US
Clinical Picture
- 80-year-old female presenting with a two-day history of diarrhoea and vomiting
- Feeling thirsty and generally unwell
- Looks tired and anxious
Findings
- Rate: 107
- Rhythm: Regular
- Axis: Normal
- Waves and intervals: Symmetrically peaked T-waves
Summary
- The EKG shows sinus tachycardia with symmetrically peaked T waves
Differential diagnosis
- Maria is an older adult with multiple comorbidities including high blood pressure, ischemic heart disease and chronic kidney disease. Maria has presented with a two-day history of diarrhoea, vomiting, thirst and an EKG showing sinus tachycardia with peaked T waves. This history would indicate dehydration which, combined with her chronic kidney disease, could lead to electrolyte imbalances. This information, together with the peaked T waves seen in Maria’s EKG, should lead a clinician to suspect hyperkalemia.
Management
- The most appropriate initial management of Maria’s presentation would be to administer IV calcium. This is usually given in the form of calcium gluconate (30mls of 10% solution – equivalent to 6.8 mmol) or calcium chloride (10mls of 10% solution – equivalent to 6.8 mmol). As you can see, the doses slightly differ, so ensure you check your local protocols and drug stocks to see which is used in your area of practice.
- IV calcium acts to stabilize the cardiac cell membrane and prevent dangerous arrhythmias which can be caused by hyperkalemia. This is the most important first step to consider in treating hyperkalemia, particularly in patients with cardiac symptoms (such as chest pain and palpitations) or EKG changes. It is important to remember that whilst IV calcium does protect the heart, it does not lower the blood levels of potassium and further treatment is required. This will usually entail nebulized albuterol, and IV glucose or dextrose with insulin which temporarily shifts potassium into the cells and out of the blood stream. After this, fluids and calcium binding agents are often given to help patients flush out the excess potassium. However, protecting the heart is still the most crucial step and this is why IV calcium remains the most appropriate answer in this case.